


Background:
Red blood cell exchange (RBCX) is an effective therapy in the treatment of different hemoglobinopathies. The University of Nebraska Medical Center (UNMC) established a chronic RBCX program in November 2015, which took care of patients with multiple hemoglobinopathies. In this study, we aim to evaluate the outcomes of this program.
Methods:
This is a retrospective study. After an IRB approval, we reviewed the charts of patients who were enrolled in the chronic RBCX program between 11/2015-7/2020 at UNMC. Data was collected to evaluate indications of RBCX, types of hemoglobinopathies, hemoglobinopathies' complications before and after the enrollment in the program, and assessment of hospital visits before and after enrollment in the program.
Results:
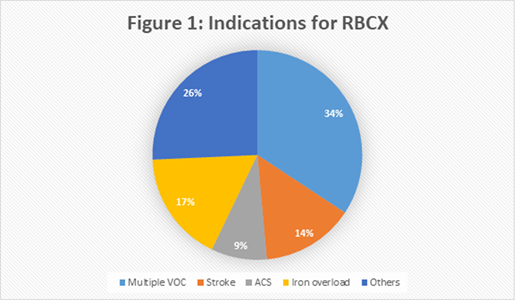
In November 2015, the chronic RBCX program was established in Nebraska. Since the start, 24 patients came through the program and 20 patients are still actively enrolled and undergoing regular exchange transfusions. The four patients who left the program did it for the following reasons: moving out of state, stem cell transplant and change to different treatment modality. Four of 24 patients were beta thalassemia patients (two of them with combined HbE/beta thalassemia). Twenty patients had sickle cell disease with two of them having combined beta thalassemia and HbS and one with alpha thalassemia and HbS. The indications ranged from history of stroke, intracranial vascular stenosis, acute chest syndrome (ACS), iron overload, multiple vascular occlusive crises (VOC) and intolerance of medications with most of the patients having multiple indications from the list above (Figure 1). There are several positive outcomes from being on the program. In the patients who had been on the program for at least one year (n=11), nine started the program with iron overload and all of them had a significant decrease in serum ferritin (average 751 ng/mL) with three patients returning to normal range. In the patients who had been in the program at least six months (n=16), 13 patients started with iron overload with five returning to normal range and average decrease in ferritin of 585 ng/mL. Another positive outcome is the number of emergency department (ED) visits for pain crisis. We noted reduction in ED visits in all patients who were in the program for at least six months (n=14), with the exception of one patient where the visits were likely the part of drug seeking behavior. In fact 12 of 13 patients had one or no ED visits within one year after starting on the chronic exchange program having had from 2-11 visits a year prior. None of the patients in the program experienced more severe complications of sickle cell disease, like stroke and acute chest syndrome, while on the program. Due to high volumes of transfusion, there is a big concern about developing red blood cell antibodies in sickle cell disease patients who in general have higher red blood cell antibody burden. Out of 24 patients in the program, six had pre-existing antibodies. For the duration of the program, no new alloantibodies were discovered in the chronically exchanged patients despite high transfusion volumes (range 14L-30L/year). The transfused blood was matched for Rh and Kell antigens for the patients with no antibody history. The patients with previous antibody history had additional matching for the antigen to which antibody was directed.
Conclusion:Automated chronic RBCX transfusion program is safe to perform. It leads to significant reduction in volume overload and ED visits. Performing high volume transfusions outside of acute sickle cell crisis and with Rh and Kell matched units prevents formation of RBC antibodies
Gundabolu:BioMarin:Consultancy;Bristol Myers Squibb pharmaceuticals:Consultancy.
This icon denotes a clinically relevant abstract

